




Bleeding from the nose is also known as called EPISTAXIS.
Approximately 50% population experience nosebleeds in their life but it is serious enough to seek medical consultation in less than 10% only.
There is no age bar. Children usually have mild anterior nasal bleeding while the elderly have profuse posterior nose bleeding.
Males are affected more than females but after the age of 50 years both the sexes are affected equally.
TYPES OF NOSE BLEED
There are two kinds of nosebleeds- ANTERIOR and POSTERIOR
ANTERIOR NOSE BLEED
– In the anterior nosebleed, blood flows from the FRONT OF THE NOSE out through the nasal opening.
– It is more common than posterior nasal bleeding.
– The common sites for Anterior Nose bleed are –
- Little’s area (it’s a small area situated in the front of the nasal septum), and
- Anterior part of LATERAL NASAL WALL.
– It is usually mild and may be controlled by local pressure like pinching of the nose or anterior packing.
– It mostly affects children and young adults and the most common cause is TRAUMA/NOSE PICKING.


POSTERIOR NOSE BLEED
– In a posterior nasal bleed, blood flows down the back of the throat, as bleeding occurs in the back or the deeper part of the nose.
– Posterior nasal bleeding is LESS common but MORE severe.
– It mostly occurs spontaneously.
– Most of the patients are more than 40 years of age.
– Bleeding can be so severe that the patient might require hospitalization and postnasal packing.
– The blood, which can be seen in the pharynx, is swallowed by the patient and then later on vomited out as coffee-colored vomitus.
– The bleeding site is difficult to localize as it lies is mostly in the deeper part of the nasal cavity.
– The most common cause of posterior nasal bleed is HYPERTENSION and ARTERIOSCLEROSIS.

AREAS IN NOSE RESPONSIBLE FOR ANTERIOR NOSE BLEED-
## Little’s Area/Kiesselbach’s Plexus is mainly responsible for anterior “ARTERIAL” nasal bleed

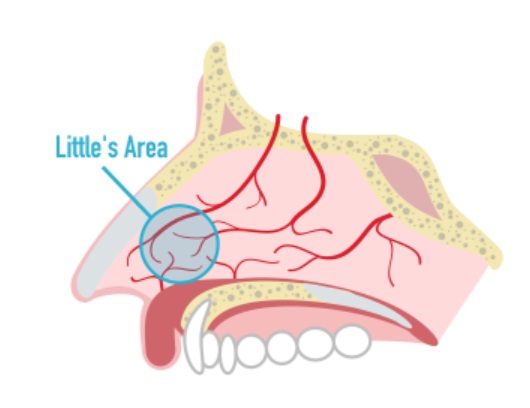
LOCATION OF LITTLE’S AREA – Little’s area is situated in the anterior-inferior part of the nasal septum and is supplied by branches of both external and internal carotid arteries.
– The 4 arteries, the branches of which anastomose richly and form a vascular plexus (Kiesselbach’s plexus) in this region are:
1. Anterior ethmoidal artery
2. Septal branch of the Superior labial artery
3. Septal branch of the Sphenopalatine artery (most common culprit)
4. Greater palatine artery
– This vascular area is the most common site of “ARTERIAL” nosebleeds in children and young adults.
– It commonly gets dried due to the effect of the inspiratory current of excessive DRY AIR or winter COLD AIR and also is easily traumatized due to frequent picking (fingering) of the nose.
– SPHENOPALATINE ARTERY is also known as the “ARTERY OF EPISTAXIS/NOSE BLEED”
## Retrocolumellar vein responsible for anterior “VENOUS” nasal bleed
LOCATION OF RETROCULUMELLAR VEIN – It runs vertically downward just behind the columella of the nose and crosses the floor of the nose.
– It is a common source of “VENOUS” bleeding in young people.
AREAS IN NOSE RESPONSIBLE FOR POSTERIOR NOSE BLEED-
WOODRUFF’S PLEXUS
– This is a plexus of large thin-walled veins, hence responsible for venous posterior bleed.
– Woodruff’s plexus is located on the lateral wall of the nasal cavity below the posterior end of the INFERIOR NASAL TURBINATE.
CAUSES OF NASAL BLEED
– Causes of epistaxis can be divided into –
- LOCAL CAUSES, and
- GENERAL CAUSES
– The most common cause of nosebleeds in children is repeated FINGERNAIL TRAUMA to the Little’s area.
– In elderly people, the most common cause is Atherosclerotic changes and Hypertension.
– In many cases, no obvious cause is ascertained, and then it’s termed as IDIOPATHIC.
– In vicarious menstruation, a nosebleed occurs at the time of menstruation.
LOCAL CAUSES of nose bleed are-
a. TRAUMA eg.
- Fingernail trauma (Nose picking, the MOST COMMON CAUSE)
- Injuries of the nose (accidental, homicidal, surgery)
- Maxillofacial trauma
- Head injuries
- Nasal intubation
- Foreign bodies stuck inside nose (common in children)
- Rhinolith (stone formation inside nose)
- Blowing of nose too hard
- Violent sneezing
b. INFECTIONS eg.
- Rhinitis
- Nasal vestibulitis
- Sinusitis
- Rhinosporidiosis
- Granulomatous lesions (Tuberculosis, Syphilis, Sarcoidosis, Wegener’s granuloma)
- Atrophic rhinitis
- Maggots
- Leeches
- Neglected foreign body inside nasal cavity
c. NEOPLASMS eg.
(i) Benign Neoplasms like –
- Hemangioma
- Inverted papilloma
- Juvenile nasal angiofibroma
- Aneurysms
(ii) Malignant neoplasms like –
- Epidermoid carcinoma
- Adenocarcinoma
- Sarcoma
- Esthesioneuroblastoma aka Olfactory neuroblastoma
d. ENVIRONMENTAL eg.
- High altitudes
- Sudden decompression (Caisson’s disease)
- Chemicals
- Pollution
e. Drugs eg.
- Prolonged use of Nasal sprays and drops of antihistaminics and steroids like Oxymetazolie, xylometazoline, fluticasone, mometasone etc.
- Sniffing of cocaine
f. MISCELLANEOUS eg.
- Septal deformities
- Septal perforation
GENERAL CAUSES of nose bleed are-
a. CARDIOVASCULAR eg.
- Hypertension,
- Mitral stenosis,
- Congestive heart failure
- Eclampsia of pregnancy
b. HAEMOPOIECTIC:
- Aplastic Anaemia
- Leukaemia
- Thrombocytopenic and vascular purpura
- Haemophilia A
- Haemophilia B (Factor IX deficiency or Christmas disease, is the second most common type of hemophilia)
- Polycythemia vera
- Multiple myeloma
c. NUTRITIONAL eg.
- Malnutrition
- Scurvy
- Alcohol abuse
- Vitamin A, D, C, E and K deficiencies
- High doses of vitamin E
d. BLOOD VESSELS eg.
- Arteriosclerosis
- Collagen diseases
- Hereditary hemorrhagic telangiectasia (HHT)
e. LIVER DISEASE eg.
- Hepatic cirrhosis (deficiency of Factor 2, 7, 9, and 10)
f. KIDNEY DISEASE eg.
- Chronic nephritis
- Renal failure
g. DRUGS eg.
- Nonsteroidal anti-inflammatory drugs (NSAIDs) such as Ibuprofen and Diclofenac
- Anticoagulant therapy such as Ecospirin, Warfarin, Heparin and coumadin
h. ACUTE INFECTIONS eg.
- Dengue fever
- Influenza
- Measles
- Chickenpox
- Whooping cough
- Rheumatic fever
- Infectious mononucleosis
- Typhoid
- Pneumonia
- Malaria
DIAGNOSING NOSE BLEED
A case of nose bleed has to undergo 3 stages so as to come to a confirmatory diagnosis of cause-
- HISTORY
- EXAMINATION
- INVESTIGATIONS
HISTORY


Complete history includes the following questions:
1. Which is the Side of bleeding?
2. Which side is the worst side if bleeding occurs from both nasal cavities?
3. Patient is asked for symptoms of posterior nasal bleeding such as coughing out of clotted blood or coffee-colored vomiting.
4. Ask for any Precipitating events such as trauma, acute infection, nasal drops and sprays, and surgery.
5. What is the Duration and Amount of bleeding?
6. Any Risk factors if present such as hypertension, leukemia, hemophilia, purpura, congestive heart failure, renal failure, and liver dysfunction and their medications?
7. If the patient is using any drugs such as Ecospirin, Aspirin, Warfarin, Heparin, NSAIDs (ibuprofen), antiplatelet drugs, high doses of vitamin E?
8. Past history of bleeding and what was the treatment given?
9. Family history of bleeding tendencies such as hemophilia.
10. Ask about Occupational history and residential address as people who reside in places with hot climate/dry air or very cold winters, or who work at places that have overall high temperatures like glass blowing, steam engines, or ovens tend to have a nasal bleed.
(Both excessive hot/dry or excess cold weather can cause epistaxis)
EXAMINATION
1. Examination should include vital parameters, complete ear, nose, and throat examination, general features, and systemic examination.
2. The examination is often treatment-oriented hence the doctor tries to locate the cause and site of bleeding.
3. The local anesthesia (4% xylocaine), decongestants (oxymetazoline or xylometazoline), and mild sedation make the nasal examination as well as the patient comfortable.
4. Clots need evacuation by forceps and suction.
- The patient can be asked to blow the nose or cough, which helps in cleaning the nose and throat by bringing out the large clots.
5. Vital signs and the patient’s mental status need constant attention if the patient is actively bleeding during the physical examination.
6. Some patients may require an examination under general anesthesia.
7. Posterior nasal examination in postnasal bleeding needs a nasal endoscope.
8. Nasal endoscope also helps in localizing the site of anterior nasal bleeding.
INVESTIGATIONS
Recurrent and profuse nosebleed cases need the following investigations. The investigations might differ as per the patient’s requirement.
1. Complete blood count: To look for Anaemia, leukemia, and thrombocytopenia.
2. Bleeding and Coagulation profile:
- Bleeding time (BT)
- Clotting time (CT)
- Prothrombin time (PT)
- Activated partial thromboplastin time (PTT/APTT)
- INR
3. Radiological investigations:
- Computed tomography (CT) of face/nose/paranasal sinuses
- Magnetic resonance imaging (MRI) or Magnetic resonance angiography (MRA) of face/nose/paranasal sinuses.
HOW TO TREAT A NOSEBLEED?
(I) HOME TREATMENT
(II) DRUGS/MEDICINES
(III) NASAL CAUTERY
(IV) ANTERIOR NASAL PACKING
(V) POSTERIOR NASAL PACKING
(VI) SURGERY
(I) HOME TREATMENT
– Patients and their relatives are given the following advice if bleeding occurs at home:
1. Avoid frequent cleaning of the nose with tissue paper or finger.
2. Maintain proper nasal hydration with saline nasal drops, saline gels, and ointment eg. Nasoclear® nasal drops/nasal wash, Nasoclear® nasal gel, etc.
3. Increase ambient humidity with a bedroom HUMIDIFIER.
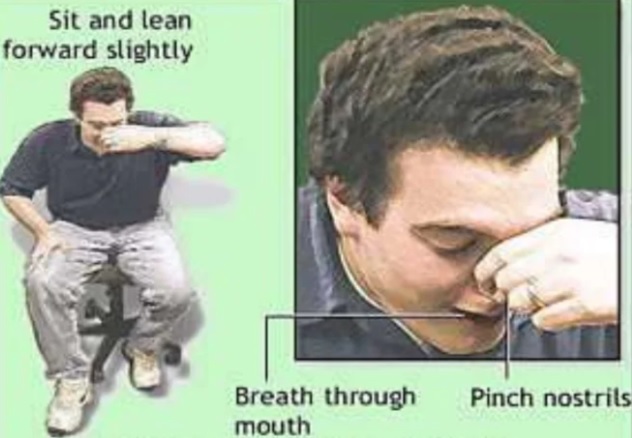
4. Do the TROTTER’S MANEUVER, where the patient sits and leans a little forward over a basin to spit any blood.
The patient breathes quietly from the mouth.
5. It should be followed by the HIPPOCRATIC MANEUVER, where the nose is pinched with the thumb and index finger for about 10 minutes in the same leaning forward position over the basin.
– It usually stops the bleeding from Little’s area which is the most common site of ANTERIOR nose bleeding.

6. Don’t lie down when trying to stop an active nosebleed.
– Lying down can result in swallowing blood and can irritate your stomach.
7. Release your nostrils after 10 minutes and check to see if the bleeding has stopped.
8. Repeat these steps if bleeding continues.
9. Place a small piece of cotton soaked in decongestant nasal drops. eg. Xylometazoline, or Oxymetazoline.
– (THIS IS NOT ADVISED FOR HYPERTENSIVE PATIENTS, as the decongestant nasal drops might further increase the blood pressure)
10. If the patient is elderly or be it any reason that patient cannot lean forward, no further than 45° leaning back is allowed.
11. Cold compresses or ice-cold water directly over the bridge of the nose results in reflex vasoconstriction and can stop bleeding.
11. Report to the doctor if bleeding does not stop.
(II) DRUGS / MEDICINES
Only under the supervision and prescription of a doctor medicine like TRANEXAMIC ACID and ETAMSYLATE can be used. These come in oral as well as injectable forms.
Tranexamic Acid is an antifibrinolytic. It works by preventing the breakdown of blood clots and controls excessive bleeding. eg. Tranexa®, Tranostat®, Pause®, etc.
Ethamsylate is a hemostatic. It works by increasing the ability of platelets to stick together and form blood clots. eg. Sylate®, Ethasyl®, etc.
ANTIHYPERTENSIVES to control blood pressure. Daily monitoring of blood pressure at home should be done using a BP machine.
(III) NASAL CAUTERY
(Chemical cautery or Electrocautery)
- Chemical cautery
– Done with a bead of SILVER NITRATE (2%) is helpful in cases of mild bleeding.
– The tip of the silver nitrate stick should be held in contact with the bleeding site for several seconds.
– The cauterized area should become grayish-white in color.
- Electrocautery (monopolar, bipolar or suction cautery)
– It is employed in cases when chemical cautery fails or in case of severe bleeding.
– Nasal Endoscope can be used so that the posterior nasal bleeding points are seen and cauterized better under endoscopic vision.
– Complication of Electrocautery: Avoid deep and bilateral cautery as they can cause SEPTAL PERFORATION.
(IV) ANTERIOR NASAL PACKING
– Anterior nasal packing is done in cases of active anterior epistaxis when home treatment and cautery have failed.
– In cases of profuse bleeding where the site of bleeding cannot be localized, anterior nasal packing is done without trying for cauterization.
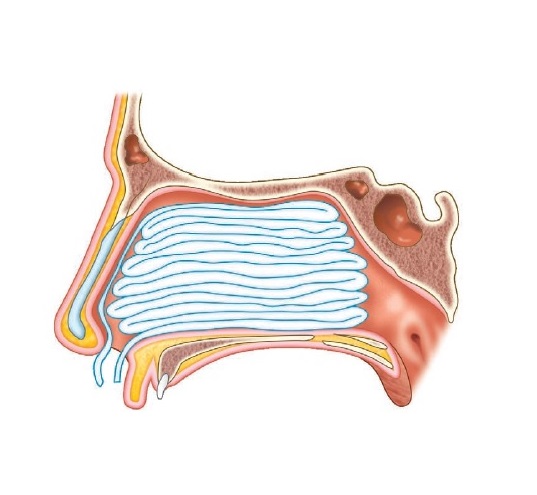
– Method of ANTERIOR NASAL PACKING (ANP): There are many materials that are available for Anterior nasal packing.
However, the 2 most commonly used materials for Anterior nasal packing are –
1st ——- is a Ribbon gauze (soaked in antibiotic ointment and liquid paraffin)
2nd—— is a Merocele®.
{ Merocele® is a compressed, dehydrated sponge composed of hydroxylated polyvinyl acetate.
After insertion in the nasal cavity, it absorbs all the blood and swells up compressing the bleeding vessels
OR
it can be rehydrated with normal saline to achieve its optimal size within the nasal cavity so as to compress the bleeding vessels.
In addition, it acts as a surface for platelet aggregation which actively encourages hemostasis.}
- The nose must be cleared of blood clots by suction and forceps.
- One meter long ribbon gauze (width 2.5 cm in adults and 12 mm in children), which is soaked in liquid paraffin and soframycin®/antibiotic ointment, is packed tightly in each nasal cavity by layering the gauze from floor to the roof and from before backward.



- Anterior nasal pack removal: Pack can be removed after 24 hours or after 2–3 days.
- Patient is started on Systemic antibiotics to prevent a infection and a potential life threatening complication which can occur due to anterior nasal packing known as TOXIC SHOCK SYNDROME.
- In addition to ribbon gauze and Merocele®, other packing materials include – – –
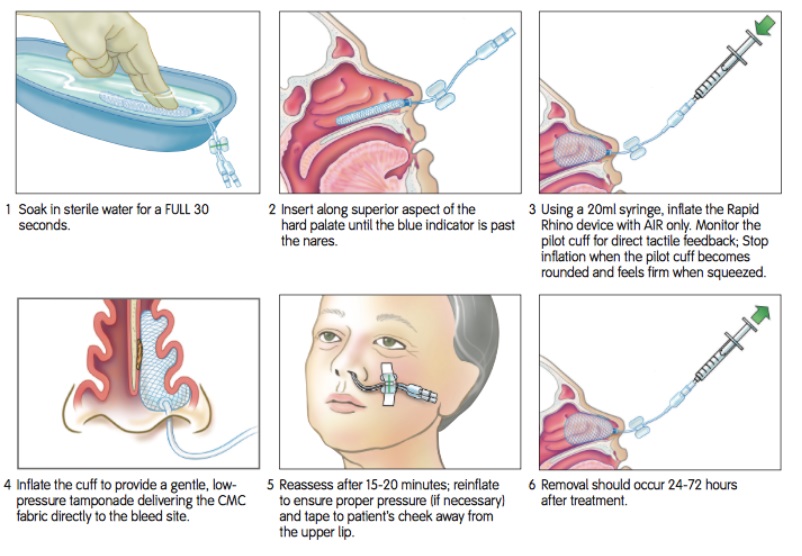
– pre fashioned anterior nasal balloons like RapidRhino®, Gelfoam®, and oxidized cellulose (Surgicel®).
The Rapid Rhino® – The Rapid Rhino® is an inflatable balloon, coated with a hydrocolloid of carboxymethylcellulose (CMC). In addition to providing direct mechanical pressure, the Rhino’s CMC functions as a lubricator (ease of application) and platelet aggregator upon exposure to water. In order to place the Rapid Rhino (activate the CMC), the device is submerged in sterile water for approximately 30 seconds prior to its insertion along the septal floor, parallel to the hard palate. A 20cc syringe is then used to inflate the balloon until the pilot cuff is rounded and firm to the touch

Video showing technique of using RapidRhino®

(V) POSTERIOR NASAL PACKING
– Posterior nasal packing is done when cauterization fails, active bleeding is still persisting and the bleeding site cannot be determined.
– Method of POSTERIOR NASAL PACKING (PNP):
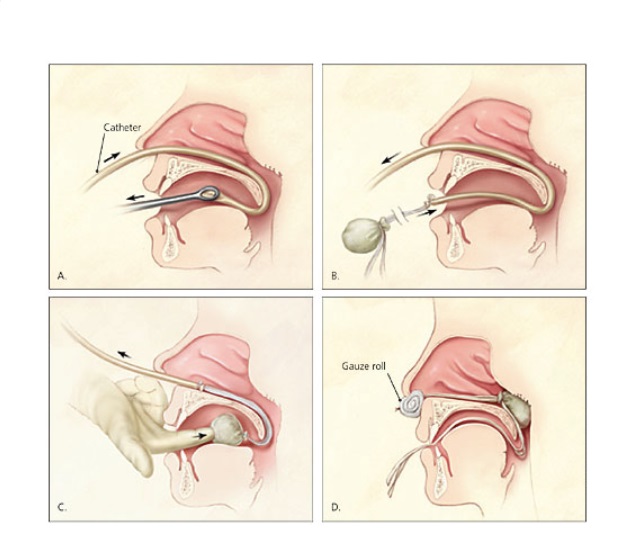
(A) Gauze:
– This is an obsolete method but still followed at some institutions. Earlier PNP was done using a piece of gauze is rolled into the shape of a cone.
– Then three silk ties are tied to this cone-shaped gauze.
– A rubber catheter is passed through the nose. Its pharyngeal end is brought out from the
mouth and the silk threads of the postnasal pack are tied to it. The catheter along with the silk threads is gradually withdrawn from the nose and the postnasal pack tied with silk
threads is guided into the nasopharynx with the index finger. The anterior nasal cavity is now also packed.
– The silk threads are tied over a dental roll. The third silk thread, which is cut short, hangs in the oropharynx and helps in the easy removal of the postnasal packing.

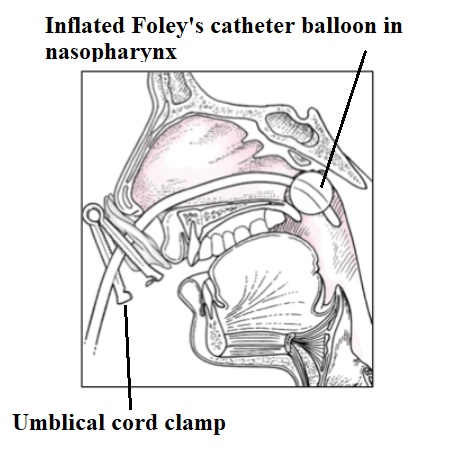
(B) FOLEY’S CATHETER:
– Many ENT surgeons use a Foley catheter (size 10, 12, or 14 French) for posterior nasal packing.
– Catheter is lubricated with xylocaine jelly and advanced until its tip and the balloon are in the nasopharynx.
– The Foley’s catheter balloon is then filled with approximately 10-15cc of saline and traction is applied anteriorly until the balloon sits firmly against the posterior nasal choana.
– Anterior traction is maintained with the placement of an umbilical cord clamp at the nasal ala.
– If hemostasis is still not achieved status post placement of the Foley catheter, anterior nasal packing using ribbon gauze as mentioned above is utilized as an adjunct.
– Appropriate application of the umbilical cord clamp is essential to prevent the complication of pressure necrosis of ala of the nose. The umbilical clamp should never be affixed directly over the nasal ala.

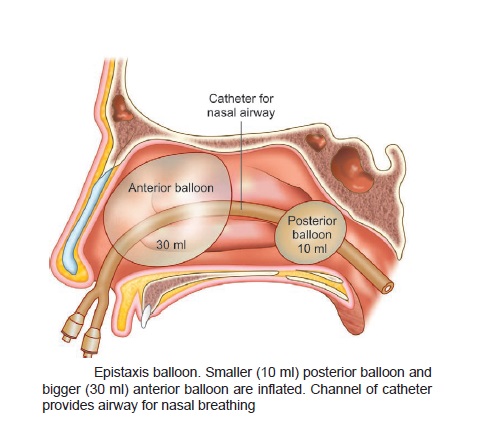
(C) NASAL BALLOON:
The current variety of nasal balloon has two bulbs, one lies in postnasal space while another remains in the nasal cavity.
The Epistat or Storz T3100® – As an alternative to the Foley catheter, the Epistat or Storz t3100® is a device with anterior and posterior balloons for the control of epistaxis. The device is inserted until the posterior balloon enters the posterior nasal cavity, inflated with 5-10cc of saline, and then pulled forward until snug. The anterior balloon is then filled with 15-30cc of saline and secured with an umbilical or c-clamp at the nasal ala.

(VI) SURGERY
When all the above-mentioned methods fail, then only surgical intervention is left to control the nosebleed.
It involves LIGATION of the culprit bloodvessels like-
- Ligation of External carotid artery
- Ligation of Internal Maxillary artery
- Ligation of Ethmoidal arteries
OR
Septoplasty/ Submucous resection is done.
– This surgery requires elevation of the mucoperichondrial/mucoperiosteal flaps from the nasal septum with excision of a part of the septum/septal spur.
– When these flaps are repositioned to their original position, they heal by fibrosis.
– This fibrosis leads to results in fibrosis and constriction of blood vessels and hence stoppage of bleeding.
OR
In cases of Hereditary hemorrhagic telangiectasia or Osler-Weber-Rendu Disease, where the anterior part of the nasal septum is involved and causes recurrent episodes of profuse bleeding.
SEPTODERMOPLASTY is performed, where the anterior part of the septal mucosa is excised and replaced by a split skin graft.
THANKS
WATCH INTERESTING ENT-related VIDEOS ON MY YouTube CHANNEL…..Dr.Sharad ENT Videos
MEDICAL ADVICE DISCLAIMER:
This blog including information, content, references, and opinions is for informational purposes only.
The Author does not provide any medical advice on this platform.
Viewing, accessing, or reading this blog does not establish any doctor-patient relationship.
The information provided in this blog does not replace the services and opinions of a qualified medical professional who examines you and then prescribes medicines.
And if you have any questions of medical nature, please refer to your doctor or the qualified medical personnel for evaluation and management at a clinic/hospital near you.
The content provided in this blog represents the Author’s own interpretation of research articles.