
CSF Rhinorrhea Symptoms is the flow of cerebrospinal fluid from the nose which can occur spontaneously or because of varied aetiological factors.
Usually, the sites of CSF leak are cribriform plate, frontoethmoid, and sphenoid sinuses which have an intimate relationship with the nasal cavity.
Cerebrospinal fluid (CSF) rhinorrhea results from a direct communication between the CSF-containing subarachnoid space and the paranasal sinuses.
Because it may serve as a path for the spread of bacterial pathogens and other microorganisms, CSF rhinorrhea may lead to meningitis and intracranial infections, which carry significant morbidity even nowadays.
Over the past three decades, the optimal treatment strategy has undergone significant evolution as minimally invasive, endoscopic techniques have gained
acceptance and supplanted more traditional techniques, which require external incisions and/or craniotomy.
AETIOLOGY
1) Traumatic (immediate and delayed):
a) Head injuries, temporal bone fracture, and maxillofacial traumas.
b) Surgeries of frontal, ethmoid and sphenoid sinus, hypophysectomy, endoscopic sinus surgery.
3) Congenital defects:
a) Congenital dehiscences of the nasal roof
b) Encephalocele.
2) Traumatic
a) Fracture of anterior cranial fossa in head injury cases (most common cause)
b) Transnasal hypophysectomy
c) Intranasal ethmoidectomy
d) Frontoethmoid mucocele operation
e) Functional endoscopic sinus surgery (FESS).
The rate of CSF leak complication during endoscopic sinus surgery has been reported as 0.5%.
3) Spontaneous
a) Raised intracranial tension
b) Hydrocephalus
c) Destructive or skull base erosive lesions like granulomas, osteomyelitis, etc.
d) Intracranial neoplasms such as tumors of the pituitary and olfactory bulb, large osteomas of frontoethmoid region, skull base neoplasms such as sinonasal and nasopharyngeal cancers.
4) Idiopathic
Sites and Pathways for CSF Leak –
1) Anterior cranial fossa CSF:
It reaches the nose through the cribriform plate, ethmoid air cells, or frontal sinus.
2) Middle cranial fossa CSF:
It reaches the nose through the sphenoid sinus.
3) Otorhinorrhea:
In transverse temporal bone fracture, CSF enters into the middle ear and then comes to the nasopharynx and nose through the Eustachian tube. The middle ear may show fluid and conductive hearing loss.
CLINICAL FEATURES
1) Unilateral, clear, watery dripping on looking downwards which increases on coughing, sneezing, or exertion.
2) History of meningitis in the past.
3) History of trauma or operation on the nose/PNS or nasopharynx for any mass.
DIAGNOSIS
The patient presents with dribbling of clear fluid from the nose on bending or straining. CSF rhinorrhea should be differentiated from the usual nasal discharge of rhinitis and sinusitis (See Table)
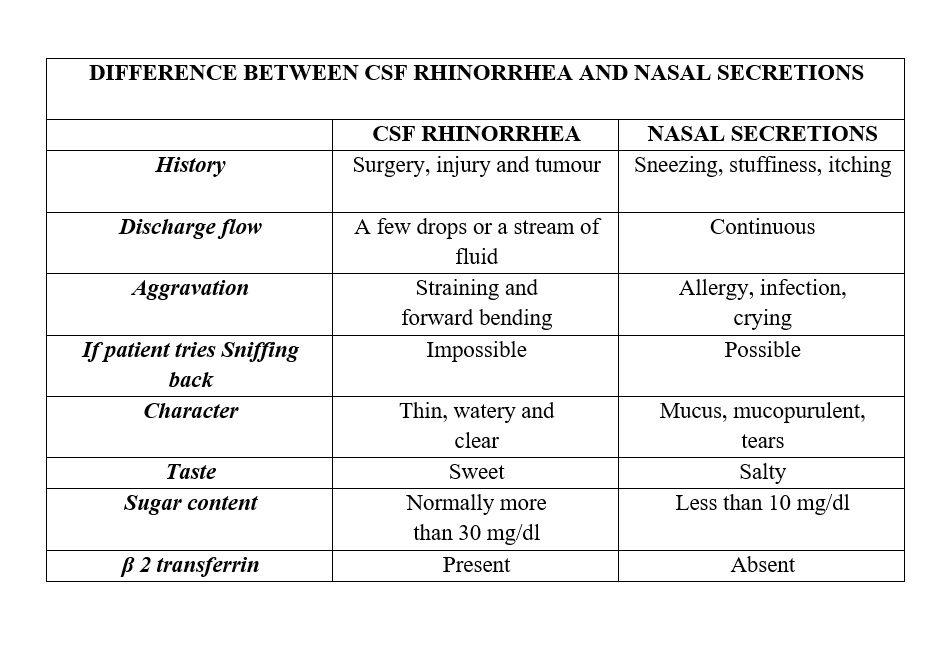
1) Physical Examination: CSF remains clear when standing in a test tube, whereas nasal discharge leaves sediment because of mucus and other proteins.
2) Handkerchief test: Nasal discharge stiffens the handkerchief while CSF does not. CSF does not stiffen the handkerchief due to the absence of mucin on drying.
3) Glucose content: Oxidase-peroxidase paper strips or biochemical tests will show the glucose content of CSF.
Compare with sugar in CSF obtained from lumbar puncture as sugar is reduced in cases of meningitis.
4) β2 transferrin (Beta 2 transferrin): It is specific for CSF and confirms the diagnosis of CSF leak.
5) Electronic nose: This novel strategy can distinguish between CSF and serum.
6) Double ring sign or target sign: In traumatic cases, when CSF is mixed with blood, double ring sign (or target sign) helps in diagnosis. Discharge is placed on a piece of filter paper, which shows a central spot of blood and peripheral halo of CSF that spreads more and faster than blood.
Complications of CSF Leak
1) Meningitis and intracranial infections.
2) Pneumocephalus and secondary brain compression.
Localization of CSF Leak (CSF Tracers)
Site of leak can be seen in high resolution CT, thin coronal cuts with bone window as HRCT can show the area of the bony defect from where the CSF is leaking.
Intrathecal agents, which are used for localizing the site of CSF leaks, include visible dyes, radionuclide markers and radiopaque dyes.
a. Intrathecal fluorescein:
Injection fluorescein 10% 0.1 ml diluted in patient own CSF is infused slowly over 30 minutes. Nasal endoscopy identifies the characteristic green color of the fluorescein in nose and sinuses at the site of CSF leak.
b. Radionuclide cisternography:
Radionuclide is injected intrathecally and pledgets of cotton are placed close to the suspected sites of CSF leak such as olfactory slit (cribriform plate), middle meatus (frontal and ethmoidal sinuses), sphenoethmoidal recess (sphenoid sinus) and Eustachian tube (temporal bone). Monitoring of the distribution of the tracer is done with a scintillation camera. These pledgets are assayed for tracer 12–24 hours later with a gamma counter.
c. CT cisternography:
CT is done after intrathecal administration of radiopaque contrast (metrizamide), which shows the presence of CSF leak.
d. MRI cisternography:
It is a non-invasive and non-ionizing technique. Heavily T2 weighted image with fat suppression and video reversal provides a means to image CSF.
Treatment
The cause of CSF rhinorrhea needs attention and needful treatment.
A. Early traumatic CSF rhinorrhea:
These are managed conservatively by:
1) Placing the patient in strict bed rest and head elevation (semi-sitting position).
2) Patient is advised to avoid nose blowing, sneezing, coughing, and straining.
3) Stool softeners.
4) Prophylactic antibiotics prevent meningitis.
5) If needed subarachnoid drainage through a lumbar catheter.
6) Acetazolamide and mannitol decrease intracranial pressure.
7) Nasal packing and drops are NOT used.
B. Persistent CSF rhinorrhea:
These patients need surgery. The repair can be done by–
1) Intracranial approach: Done by neurosurgeons via anterior cranial fossa approach by fascia lata or synthetic mesh, if spontaneous healing does not occur.
2) Nasal endoscopic approach: Done by ENT surgeons. It is usually preferred in leaks from the frontal sinus, cribriform plate, ethmoid, and sphenoid sinuses.
Thank You
MEDICAL ADVICE DISCLAIMER:
This blog including information, content, references, and opinions is for informational purposes only.
The Author does not provide any medical advice on this platform.
Viewing, accessing, or reading this blog does not establish any doctor-patient relationship.
The information in this blog does not replace the services and opinions of a qualified medical professional who examines you and prescribes medicines.
If you have any questions of a medical nature, please refer to your doctor or the qualified medical personnel for evaluation and management at a clinic/hospital near you.
The content provided in this blog represents the Author’s own interpretation of research articles.